A. Metoprolol – Explanation
Follow the above-mentioned steps for analysing an ECG
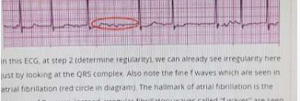
In this ECG, at step 2 (determine regularity), we can already see irregularity here just by
looking at the QRS complex. Also note the fine f waves which are seen in atrial
fibrillation (red circle in diagram). The hallmark of atrial fibrillation is the absence of P
waves. Instead, irregular fibrillatory waves called “f waves” are seen which produced a
ragged baseline. Atrial fibrillation can be differentiated from atrial flutter by the irregular
ventricular rate. Atrial flutter has a more regular ventricular rate. Atrial flutter also has
the classical “sawtooth pattern”. At times, when it is difficult to differentiate the two, we
call that “flutter-fibrillation”.
This man is an elderly man and thus rate control should be the first option (beta
blockers, calcium channel blockers or digoxin). Digoxin should be reserved for when
patient is having atrial fibrillation and heart failure together thus is not the first option
here.
These are the general rules for atrial fibrillation
- Rate control: BB or CCB or Digoxin
- Rhythm control: Amiodarone OR electrical
Rate control: BB or CCB or Digoxin —> if symptoms are not well controlled —> use combination
therapy: BB, CCB (diltiazem), Digoxin.
Rhythm control is preferred in paroxysmal atrial fibrillation, young patients, symptomatic,
younger patients presenting for first time.
If new onset atrial fibrillation + haemodynamic unstable → Emergency Electrical Cardioversion