E. Post-exposure prophylaxis – Explanation
hepatitis C and HIV. The biter is known to be a drug addict, and therefore is at a higher
risk of being infected with a blood-borne virus. This wound is considered high risk, and
post-exposure prophylaxis (PEP) should be started.
Testing for hepatitis B, hepatitis C, and HIV initially is recommended as a baseline test.
This gives us clues to whether the police officer is already positive for HIV in which case
the management differs. But the more important action is to start PEP as this can
significantly change the outcome of the incident.
The police officer will also require follow up serology blood tests at 6 weeks, 3 months
and 6 months.
All human bites should be treated with a 7 day course of oral co-amoxiclav. If the
patient has a penicillin allergy, metronidazole plus doxycycline, erythromycin or
clarithromycin.
He has had a tetanus booster within the last 5 years and therefore a further booster is
not required.
EXAMPLE OF POST EXPOSURE PROPHYLAXIS (PEP) RISK ASSESSMENT
This is an example of how Emergency Departments would perform risk assessment for
patients who may require PEP. This would differ slightly in every hospital and thus is
unlikely to be asked in the exam due to the complexity of it.
PEP Risk Assessment
Nature of incident must involve one of the following:
- Sharp injury
- Blood splash to mucous membranes (e.g. eyes/mouth)
- Contamination of broken skin with blood
- Bite or Scratch (where skin is visibly broken)
- Any of the above involving urine or body fluid that is visibly blood stained.
Risk Assessment
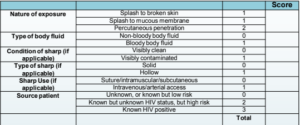
If total score is 3 or less – Prophylaxis not indicated
If total score is 4 to 7 – Consider prophylaxis
If total score is 8 to 10 – Offer prophylaxis