A. Inguinal hernia – Explanation
malesex and heavy lifting are risk factors for inguinal hernias
Traditionally it is taught that an inguinal hernia will lie above and medially to the
pubictubercle whereas a femoral hernia lies laterally and below. This is not strictly true,
as theinternal ring is always lateral to the femoral canal and a small indirect inguinal
hernia willtherefore be lateral to the pubic tubercle. A better test to differentiate the two
might beto place the finger over the femoral canal for reducible hernias and then ask the
patientto cough. When the patient coughs, a femoral hernia should remain reduced
while aninguinal hernia will reappear as an obvious swelling.
Remember, inguinal hernias has impulse on coughing or bearing down. Femoral
herniasare usually irreducible (due to the narrow femoral canal) and cough impulse
rarelydetectable.
Incarcerated hernia cannot be pushed back into the abdomen by applying
manualpressure and hence are irreducible.
Strangulated hernia are also irreducible. They are tense and red and usually followed
bysymptoms and signs of bowel obstruction
.
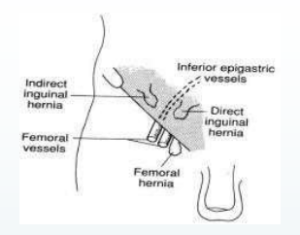
Discrimination between direct and indirect inguinal hernia by physical examination is
notvery accurate. In an indirect inguinal hernia, the protrusion passes through the
deepinguinal ring and is located lateral to the inferior epigastric artery. Whilst
traditionaltextbooks describe the anatomical differences between indirect (hernia
through theinguinal canal) and direct hernias (through the posterior wall of the inguinal
canal), thisis of no clinical relevance as the management still remains the same. The
type ofinguinalhernia in adults is usually confirmed at the operation.